Presented at Laval Virtual, April 10, 2026
Extended reality has spent years generating excitement in healthcare, and almost as many years failing to fully deliver on it. Every new device launch, from the Microsoft HoloLens 2 in 2019 to the Apple Vision Pro in operating rooms in 2024, triggers a fresh wave of headlines. At Laval Virtual 2026, Elodie Litzler, Deputy CEO and Co-Founder of Avatar Medical, offered a clear-eyed overview that cuts through the cycle: improving patient lives goes well beyond staff training, and the question worth asking is a simple but demanding one: does XR actually heal? Can it treat patients or assist doctors in providing genuinely better care?
Three Categories Worth Taking Seriously
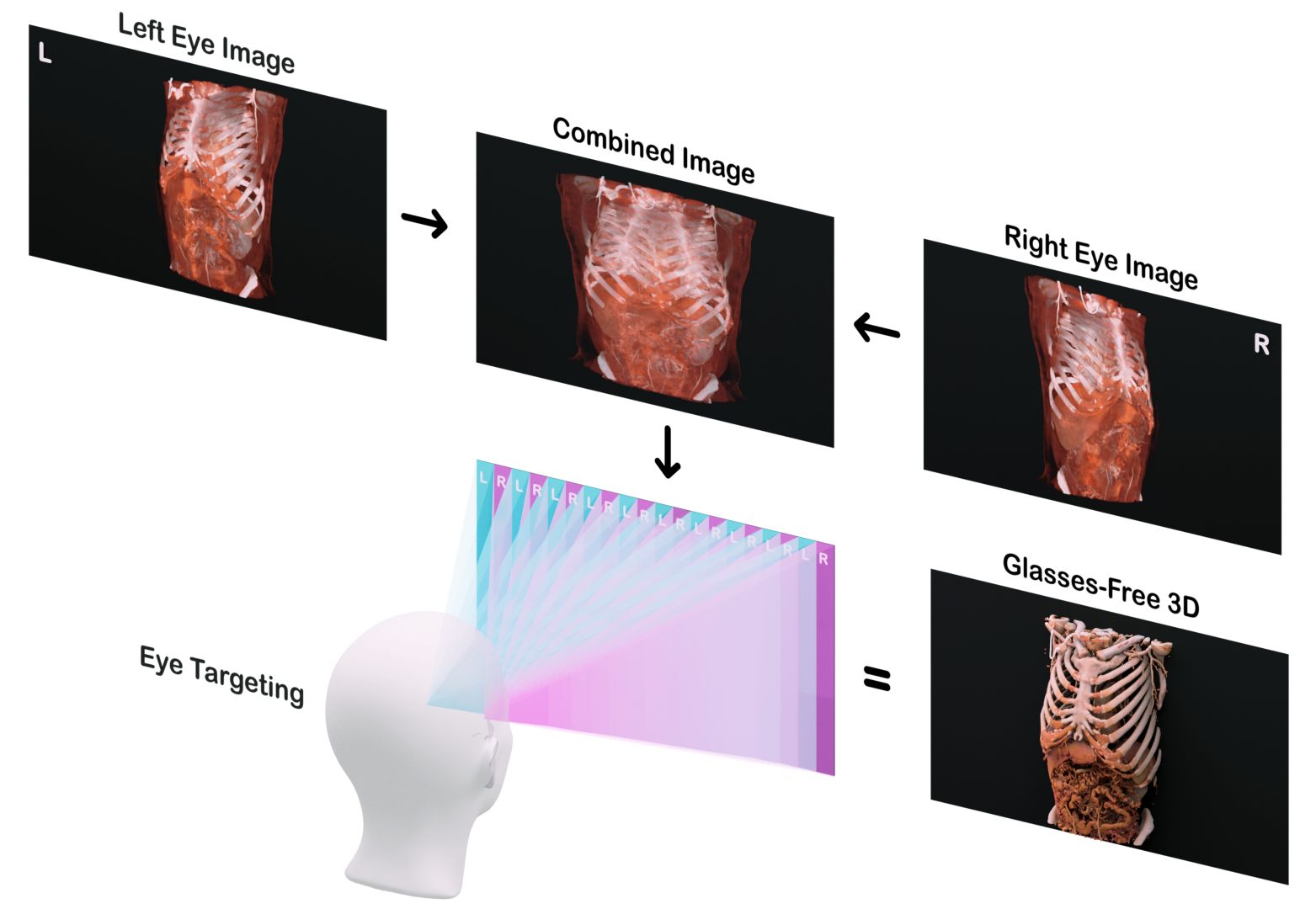
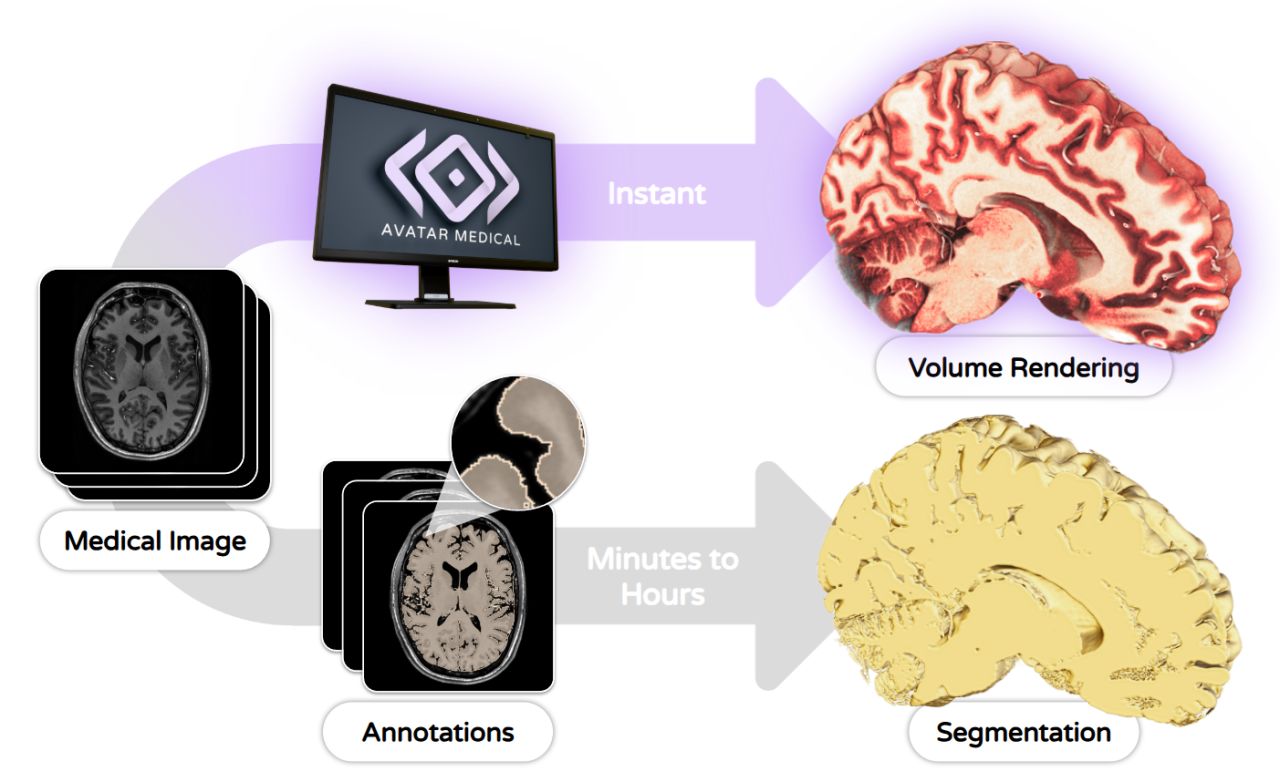
Not all healthcare XR is created equal. The presentation organized clinically meaningful applications into three categories: Digital Therapeutics, where XR delivers the treatment itself (pain management, hypnosis and anesthesia, mental health); Decision Aid, where XR assists in visualizing medical data (3D medical image visualization, smart dashboards with analytics); and Interventional, where XR assists in the realization of treatment (surgical guidance, patient positioning for radiotherapy).
The Medical Device Hurdle — and the Hardware Nightmare
Any XR solution intended for a medical purpose, treatment, diagnosis, or assisting clinical decisions, qualifies as a medical device. That means regulatory approval before market entry, and the higher the risk to the patient, the more challenging and lengthy that process becomes. The first regulatory approvals in this space date back nearly a decade: the FDA cleared the first Microsoft HoloLens-based augmented reality system for surgical use in 2018, and AppliedVR became the first VR provider to receive FDA de novo approval for a pain indication in 2021.
As of December 2025, there are 109 FDA-cleared XR medical devices across all categories, with an estimated 30–50+ CE-marked devices on the European market. Surgical AR/MR navigation leads with 51 cleared devices (~47%), followed by 3D medical image viewers at 38 (~35%), digital therapeutics at 11 (~10%), and diagnostic/other applications at 9 (~8%).
But there is a structural problem the industry rarely discusses openly: the regulatory nightmare of hardware dependency. Software as a Medical Device (SaMD) is cleared only in association with a specific list of identified hardware: head-mounted displays, 3D screens, and so on. Regulatory agencies require verification that those displays meet appropriate performance characteristics. Consumer HMD manufacturers have little incentive to run those tests for a market the size of healthcare. SaMD manufacturers, therefore, typically run the performance tests on off-the-shelf hardware themselves. The consequence is brutal: when a hardware platform reaches end of life, the entire regulatory approval dossier must be redone with the replacement device. This alone has killed or severely disrupted multiple XR healthcare companies.
Regulatory Clearance Gets You to Market. It Doesn't Mean Anyone Pays for It.
Once cleared, a product faces an entirely different challenge. In the healthcare market, the end customer (the doctor), the buyer (the hospital), and the payer (the insurance company) are three different entities with three different sets of incentives. For an insurer to pay for something, it needs to demonstrably work and deliver significant clinical value.
The evidence table as of 2026 is telling. VR for pain management has a strong evidence base: 90+ randomized controlled trials showing pain reduction in burns patients and reduction in fentanyl use (Teh et al., BMC Medicine, 2024). VR for exposure therapy is similarly well-evidenced with 30+ RCTs showing equivalence to real-world exposure (Carl et al., J Anxiety Disorders, 2019; Zeka et al., APS, 2025), though notably it is not classified as a medical device. XR for surgery has emerging evidence. The most significant milestone being the first multicenter RCT in 2025 for augmented reality-guided pedicle screw placement by Augmedics, showing a 7.3 percentage point improvement in excellent and good placement rates (p<0.0001) (Ma et al., Orthopaedic Surgery, 2025). Most prior surgical evidence, however, consists of manufacturer-associated case series.
Who Actually Reimburses, and Where
Reimbursement for XR therapies remains geographically fragmented. Germany is the most advanced, with public coverage through the DiGA pathway — Invirto (Sympatient) holds DiGA approval at €428.40 per prescription. France has a pilot program (PECAN) but no XR device reimbursement yet. Japan has a DTx reimbursement framework in place but XR-specific coverage remains early. The US is the most dynamic market: a new CPT Category III code has been created for VR therapy, and a Medicare HCPCS code was established for RelieVRx, classified as durable medical equipment at approximately $1,889 per episode, covered by Highmark and the VA. Luminopia, for pediatric amblyopia, is covered by Blue Cross Blue Shield and Highmark.
But reimbursement, when achieved, is only the beginning of commercial success. Adoption, usability, prescription rates, patient access, scalability, and international expansion are all separate and substantial challenges that follow.
When Insurance Won't Pay: The ROI Route
For categories where insurance reimbursement is not yet available, the question becomes whether hospitals can justify the cost themselves. Two levers exist: decreasing operational costs (through increased productivity or replacing more expensive equipment) and increasing revenues (more patients, more procedures). A 2026 systematic review in Frontiers in Surgery covering 30 studies (Sec. Surgical Oncology) confirmed measurable time efficiency gains across a wide range of XR-assisted procedures, but concluded this evidence base, while real, is not yet sufficient to motivate a purchase.
The revenue argument, by contrast, is more concrete in the Decision Aid category. Studies show that better 3D visualization during consultation improves patient conversion rates by approximately 20–50 percentage points. For a neurosurgeon, that translates to an estimated one additional surgery per week — over $2M per year per surgeon. And hospitals with higher patient satisfaction scores carry a meaningfully better net margin (4.7% versus 1.8%, per a Deloitte study of 3,000 US hospitals).
This points toward a broader strategic insight: patient experience is the entry point to the full continuum of care — from consultation through staff education, surgical planning, the OR, and post-op. Starting there, with a clear and immediate ROI story, creates a commercially viable beachhead that can expand.
The Path Forward
The presentation closed with a challenge that few in the XR healthcare space want to address directly. Can XR in healthcare survive absent reimbursement, on collapsed hardware platforms, through years-long hospital sales cycles, in an addressable market roughly one-hundredth the size of digital health broadly? As standalone, single-purpose companies betting everything on a single cleared device and a reimbursement code that may never come, the odds are difficult.
But that framing may be the wrong one. The companies finding traction are those that have stopped waiting for the system to validate them and started delivering value the hospital can measure today — whether through surgical precision, reduced opioid use, or a consultation room where patients actually understand what they're consenting to. The path forward increasingly runs through workflow integration, clear ROI, and building XR as a layer within broader clinical platforms rather than a destination in itself.
The technology works. The evidence is growing. The question is not whether XR belongs in healthcare, it already does, but whether the business models around it are built for the long road.