We can think of a 3D medical image as a comprehensive map of the human body. It is composed of grayscale pixels that represent different anatomy. Traditional methods of reading medical images involve examining them slice-by-slice. While this is the standard for radiology, it is fundamentally ill-suited for most medical image stakeholders, notably, patients.
Patients don’t need slices. They need information in a language that we all speak.
They need 3D.
But how can we translate these slices into a 3D experience? There are typically two approaches:
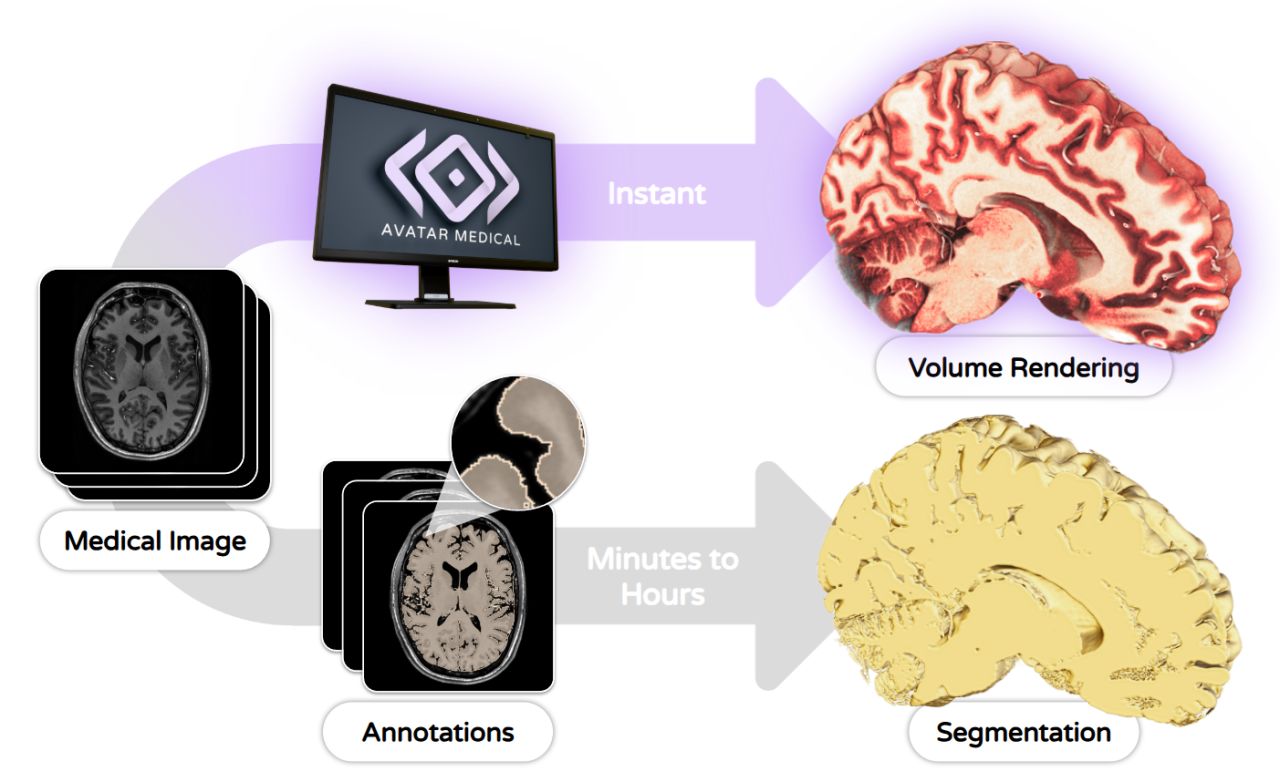
Segmentation: This involves pixel-by-pixel labeling of anatomy by hand or by algorithm. By hand, the process is laborious and subject to the annotator’s biases. By algorithm, there is no assurance that results are 100% accurate. Medical images are as diverse as patients; no algorithm can fully capture this. The typical result of a segmentation is a frozen plastic-like surface that permits measurement and quantification, but is not primed for faithful understanding of real anatomy.
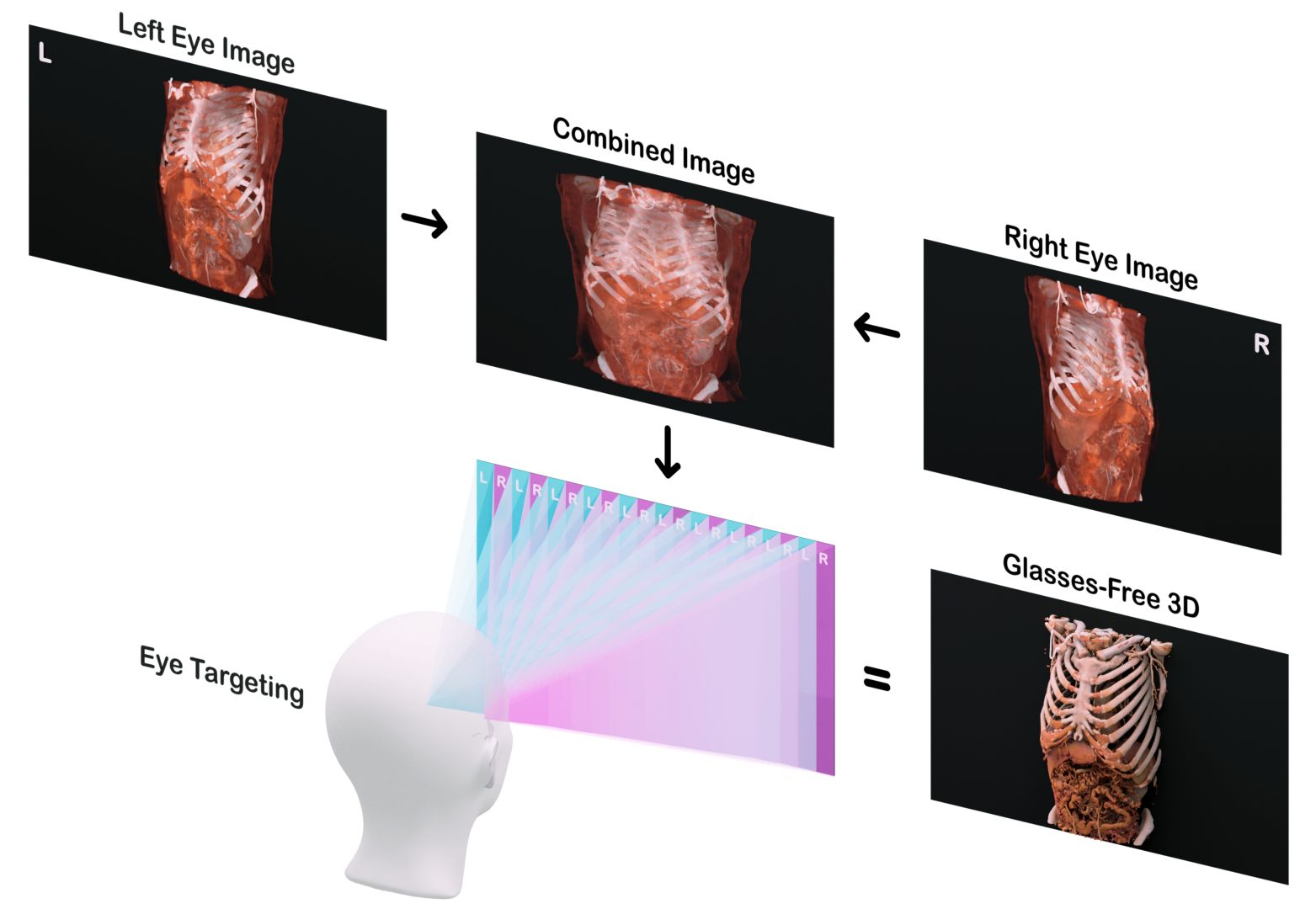
Volume Rendering: This simulates how light propagates through tissue, translating the 3D medical image data into a digital patient. In fact, it’s not really a rendering, it’s a physics simulation that captures depth, texture, lighting—nuances that mirror how we’d see anatomy in real life. Volume rendering is dynamic: it can be modified and adapted in real-time as the entirety of the image data is accessible at any given moment.
At Avatar Medical, we harness the benefits of volume rendering. We deliver instant, clinical-grade volume rendering optimized for real-world hospital deployment.
Why does this matter?
The goal is not to just show anatomy, it’s to communicate it efficiently. Whether for patient communication, surgical planning, or clinical decision-making, the fidelity of the visualization correlates to the outcome. Medicine is inherently uncertain. Segmentation, while powerful, carries implicit assumptions. It’s a product of human or algorithmic interpretation; it implies certainty where none is guaranteed.
Conversely, volume rendering is objective. It doesn’t rely on subjective labeling; it reveals structure, context, and relationships without bias. It speaks to the viewer as a viewer, not just as a radiologist.
Ultimately, the question is not simply how we visualize medical images, but rather how we make them understandable. When imaging moves from slices or simplified models to realistic, intuitive 3D avatars, it becomes a shared language. It allows clinicians to communicate more clearly, patients to grasp their own anatomy, and decisions to be made with greater confidence. In that sense, the true value of volume rendering is not technological; it’s human. It transforms medical images into shared knowledge, making medicine more collaborative.